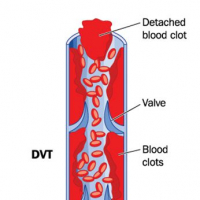
What is a DVT?
Deep vein thrombosis (DVT) is a medical condition that results in a clot forming in your veins. Most commonly these clots develop in the veins of leg, but can actually form in any vein in the body. Rudolf Virchow, a German physician from the 1800’s, came up with three categories of why people may develop clots. These are hypercoagulability (sticky blood), hemodynamic changes (blood not moving) and endothelial injury (damage to the blood vessel walls). In real life, these might occur after someone undergoes surgery, during pregnancy or on a long haul flight. However, sometimes there is no reason at all! When these clots develop, they cause the leg to swell and to become very painful. However, one of the real dangers is if the clot gets released and travels into the lungs, where it can cause serious problem by preventing blood from reaching the alveoli, which is called a pulmonary embolism (PE).
How we used to treat it
Up until recently DVTs were treated with a combination of unfractionated heparin (UFH) or a low molecular weight heparin (LMWH) and a vitamin K antagonist, usually Warfarin/Coumadin. Both heparins work by targeting an enzyme inhibitor, antithrombin III. When the heparin is bound to antithrombin III, it pretty much gives it super powers, deactivating clotting factors at 1000 times the normal speed. The end result, it becomes a lot harder for clots to form. Warfarin takes a little bit longer to work, as it targets vitamin K. Vitamin K is required in the formation of several clotting factors. Warfarin works, by binding a vitamin K epoxide reductase, which diminishes the levels of vitamin K that can actually be used.
Click here to find out more about the new Cochrane evidence by reading Pishoy's full blog on Students 4 Best Evidence.